4/26/23 - 2-Year Extension of Medicare Telehealth Flexibilities
On December 29, 2022, President Biden signed the Consolidated Appropriations Act of 2023, which includes several provisions impacting telehealth, including a 2-year extension of many COVID-19 telehealth flexibilities. In a budget bill passed previously for FY 2022, Congress had included a 151-day extension after the end of the public health emergency (PHE) for some COVID-19 telehealth flexibilities. However, with the passage of the Consolidated Appropriations Act of 2023, the following Medicare telehealth flexibilities will now last until December 31, 2024:
- Expanding originating and geographic site to include anywhere the patient is located, including the patient’s home;
- Expanding eligible practitioners qualified to furnish telehealth services, including occupational therapists, physical therapists, speech-language pathologists and audiologists;
- Delaying the in-person requirement for mental health services furnished through telehealth;
- Extending coverage and payment for audio-only telehealth services;
- Extending the Acute Hospital Care at Home (AHCAH) initiative; and requiring the HHS Secretary to publish a report comparing AHCAH programs with traditional inpatient care delivery;
- Extending the ability to use telehealth services to meet the face-to-face recertification requirement for hospice care;
- Extending the ability for federally qualified health centers (FQHCs) and rural health clinics (RHCs) to furnish telehealth services.
A notable exclusion from this 2-year extension is the Ryan Haight waiver, which has allowed remote prescription of clinically appropriate controlled substances. This waiver is still scheduled to expire with the end of the PHE, which is currently active until at least April 2023.
The Connected Health team will monitor for additional guidance, such as CMS-issued FAQ documents.
QUESTIONS?
Reach out to the Connected Health team: PennConnectedHealth@pennmedicine.upenn.edu
4/13/23 - Telehealth & Virtual Supervision of Residents/Fellows
Additional details and information about some special circumstances are available at these links.
Note: We do not qualify as a “rural area” that allows exemptions as we are in a metropolitan statistical area or MSA
Resident Supervision Requirements Under Medicare (aamc.org)
MLN006347 – Teaching Physicians, Interns, & Residents Guidelines (cms.gov)
Details: Primary Care Exception
Although under Medicare rules residents are typically supervised in-person during the critical or key portions of the service by a teaching physician, the “primary care exception” allows residents (after completing six months of residency) to furnish office/outpatient evaluation and management (E/M) visit codes of lower and mid-level complexity (99201, 99202, 99203, 99211, 99212, 99213 and annual wellness visits (HCPCS G0402, G0438, G0439) without the presence of a teaching physician. The teaching physician must be immediately available onsite to provide the necessary direction and can only supervise four residents at a time. Under this exception, the teaching physician must also review the patient’s medical history, physical examination, diagnosis, and record of tests and therapies during or immediately after each visit. The teaching physician must have no other responsibilities at the time the residents are being supervised, assume management responsibility for the beneficiaries seen by the residents, and ensure that the services furnished are appropriate.
04/22/22 – IBC telemedicine reimbursement update
On March 1, 2022 IBC notified all Network Providers, including Penn Medicine, that effective 6/1/2022, reimbursement for telemedicine services provided to IBC Commercial (non-Medicare Advantage) Members/Patients in accordance with the 7/1/2021 Medical Coverage Policy for Telemedicine Services will be reduced by 15% of the established contracted rate. This reimbursement change will not apply to IBC Medicare Advantage products or behavioral health services.
The Penn Medicine Managed Care Contracting office is working closely with IBC on potential opportunities to mitigate the impact of this policy change. We will keep the health system informed as progress is made. In the meantime, this policy will apply to Penn Medicine and reimbursement reductions will be applied for dates of service beginning on June 1, 2022.
Click here to download this memo as a PDF.
04/20/22 – IBC commercial patients - stop non-parity telephone E/M codes
The purpose of this communication is to inform all Penn Medicine Physician Providers to stop performing and billing non-parity telephone E/M codes (99441 – 99443) for IBC Commercial** patients.
**These services are able to be provided to IBC Medicare Advantage patients since IBC follows Medicare guidelines and the non-parity telephone E/M codes are covered for the duration of the PHE.
Please share this information with your clinical and administrative leadership.
BACKGROUND
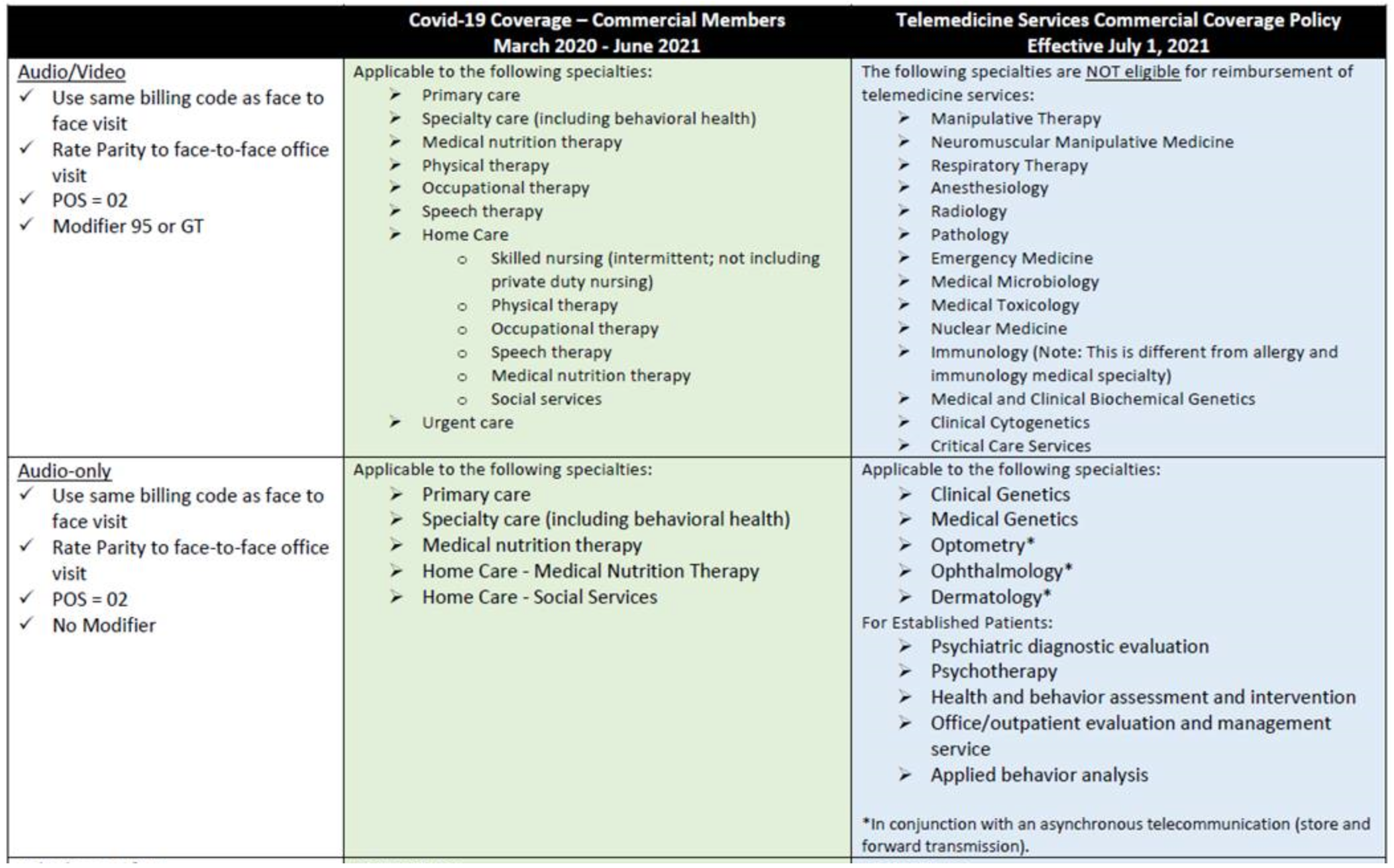
- IBC issued a Commercial (non-Medicare Advantage) Medical Coverage Policy for Telemedicine Services effective 7/1/2021. The policy provides details on which services are covered and eligible for reimbursement via telemedicine, and which are not.
- At the time the new policy was published, Penn Medicine felt it was unclear if IBC was covering/reimbursing the non-parity telephone E/M codes (99441 – 99443).
- Therefore, Managed Care Contracting requested clarification and received email confirmation indicating that the non-parity telephone E/M codes (99441 – 99443) were covered and eligible for reimbursement.
- After receiving claim denials for these services and raising concerns to IBC, Penn Medicine was notified that we had been misinformed; the non-parity telephone E/M codes are in fact neither covered nor eligible for reimbursement after 7/1/2021.
- We have been disputing this with IBC for months as we firmly believe their 7/1/2021 Commercial policy remains misleading.
- We have been unable to convince IBC of the flaw in their policy, and for this reason we believe it is important to stop performing and billing non-parity telephone E/M codes (99441 – 99443) for IBC Commercial patients.
- We will continue to pursue payment for the non-parity telephone E/M codes (99441 – 99443) provided to IBC Commercial patients up to this point as Penn Medicine was acting on the guidance provided by IBC.
- Below is a summary table that compares the Covid-19 period coverage to the new 7/1/2021 permanent Commercial policy coverage. IBC continues to pay at parity to in person office visits for all telemedicine services in the policy until 5/31/2022. A separate communication is forthcoming about the reimbursement reductions scheduled for 6/1/2022.
Click here to download this memo as a PDF.
01/11/22 – NJ telemedicine flexibilities extended
In response to the latest COVID-19 wave, telemedicine flexibilities have been extended in New Jersey. Penn Medicine practitioners who are based in Pennsylvania may continue to provide telemedicine across state lines into New Jersey for established patients only. Out-of-state telemedicine New Patient Visits are not permitted at this time. See details below:
- Practitioners without a temporary or permanent New Jersey license can have telemedicine visits with established patients located in New Jersey until May 11th, 2022. This timeline may be extended further with additional extensions of the New Jersey Public Health Emergency (PHE) and State of Emergency (SOE).
- Practitioners in the Group 2 license category with Temporary Emergency Reciprocity Licenses (TERLs) will have TERLs extended through June 30th, 2022. A TERL offers license reciprocity for both in-person and virtual care with patients located in New Jersey. Additionally, New Jersey will continue to accept new TERL applications from Group 2 practitioners while the program remains active.
- Group 2 practitioners include: Advanced practice nurse, licensed social worker, doctor of osteopathy, home health aide, licensed practical nurse, licensed alcohol and drug counselor, licensed clinical social worker, marriage and family therapist, medical doctor, professional counselor, psychoanalyst, psychologist, registered professional nurse, and respiratory care practitioner.
With the exception of the updated New Jersey telemedicine flexibility end dates outlined above, Penn Medicine’s existing out-of-state telemedicine guidance remains the same. You can always contact our team at PennConnectedHealth@pennmedicine.upenn.edu
Click here to download this memo as a PDF.
06/25/21 – Important IBC telemedicine update
The IBC permanent Commercial Telemedicine Services Policy will go into effect on 7/1/2021. There is no change at this time to the coverage for Medicare Advantage members. There is no change at this time to the expected reimbursement for telemedicine services (parity with in person visits). Coverage applies when:
- Performed by a participating provider* licensed in the State in which the individual originates the telemedicine encounter, and
- Delivered via HIPAA compliant system:
- Interactive, synchronous (real-time) two-way audio & video
- Asynchronous telecommunication (store and forward transmission) in conjunction with a synchronous audio interaction (telephone call) for Optometry, Ophthalmology and Dermatology ONLY
- Telephone communication (audio only/telephone call) for Clinical Genetics and Medical Genetics ONLY
* Certain specialties not eligible for telemedicine (e.g. Radiology, Respiratory Therapy, etc.)
More detail can be found at the links below:
- Click here for the IBC Commercial Telemedicine Coverage Policy in effect July 1, 2021
- Click here for the IBC Medicare Advantage Telemedicine Coverage Policy in effect from March 6, 2020 through the duration of the Federal Public Health Emergency.
- Click here for the IBC Commercial Telemedicine Coverage Policy in effect from March 6, 2020 to June 30, 2021.